Jan 28 2024 105 mins
Outline
Chapter 14
- Hypovolemic States
- Etiology
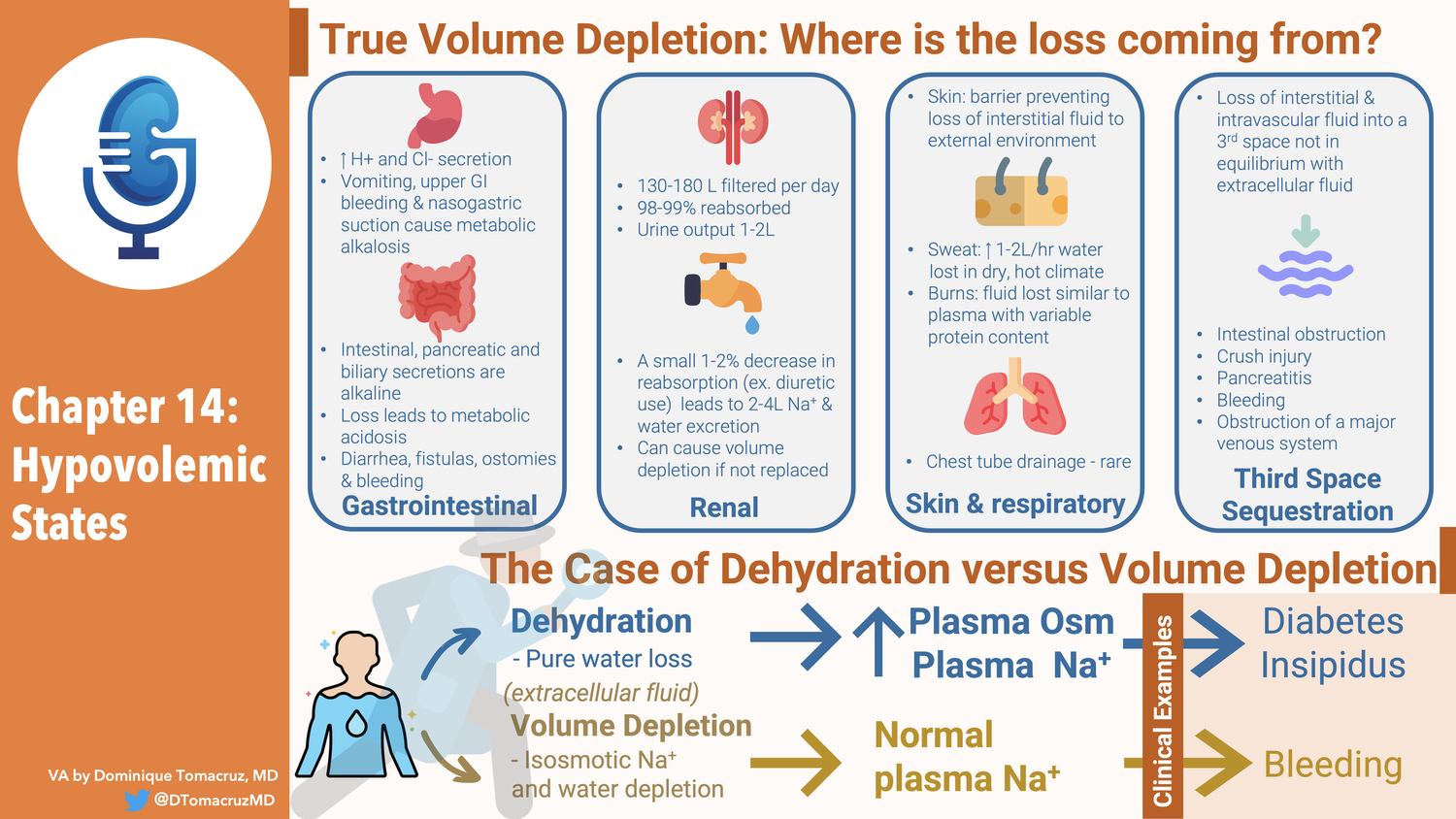
- True volume depletion occurs when fluid is lost from from the extracellular fluid at a rate exceeding intake
- Can come the GI tract
- Lungs
- Urine
- Sequestration in the body in a “third space” that is not in equilibrium with the extracellular fluid.
- When losses occur two responses ameliorate them
- Our intake of Na and fluid is way above basal needs
- This is not the case with anorexia or vomiting
- The kidney responds by minimizing further urinary losses
- This adaptive response is why diuretics do not cause progressive volume depletion
- Initial volume loss stimulates RAAS, and possibly other compensatory mechanisms, resulting increased proximal and collecting tubule Na reabsorption.
- This balances the diuretic effect resulting in a new steady state in 1-2weeks
- New steady state means Na in = Na out
- GI Losses
- Stomach, pancreas, GB, and intestines secretes 3-6 liters a day.
- Almost all is reabsorbed with only loss of 100-200 ml in stool a day
- Volume depletion can result from surgical drainage or failure of reabsorption
- Acid base disturbances with GI losses
- Stomach losses cause metabolic alkalosis
- Intestinal, pancreatic and biliary secretions are alkalotic so losing them causes metabolic acidosis
- Fistulas, laxative abuse, diarrhea, ostomies, tube drainage
- High content of potassium so associated with hypokalemia
- [This is a mistake for stomach losses]
- Bleeding from the GI tract can also cause volume depletion
- No electrolyte disorders from this unless lactic acidosis
- Renal losses
- 130-180 liters filtered every day
- 98-99% reabsorbed
- Urine output of 1-2 liters
- A small 1-2% decrease in reabsorption can lead to 2-4 liter increase in Na and Water excretion
- 4 liters of urine output is the goal of therapeutic diuresis which means a reduction of fluid reabsorption of only 2%
- Diuretics
- Osmotic diuretics
- Severe hyperglycemia can contribute to a fluid deficit of 8-10 Iiters
- CKD with GFR < 25 are poor Na conservers
- Obligate sodium losses of 10 to 40 mEq/day
- Normal people can reduce obligate Na losses down to 5 mEq/day
- Usually not a problem because most people eat way more than 10-40 mEq of Na a day.
- Salt wasting nephropathies
- Water losses of 2 liters a day
- 100 mEq of Na a day
- Tubular and interstitial diseases
- Medullary cystic kidney
- Mechanism
- Increased urea can be an osmotic diuretic
- Damage to tubular epithelium can make it aldo resistant
- Inability to shut off natriuretic hormone (ANP?)
- The decreased nephro number means they need to be able to decrease sodium reabsorption per nephron. This may not be able to be shut down acutely.
- Experiment, salt wasters can stay in balance if sodium intake is slowly decreased. (Think weeks)
- Talks about post obstruction diuresis
- Says it is usually appropriate rather than inappropriate physiology.
- Usually catch up solute and water clearance after releasing obstruction
- Recommends 50-75/hr of half normal saline
- Talks briefly about DI
- Skin and respiratory losses
- 700-1000 ml of water lost daily by evaporation, insensible losses (not sweat)
- Can rise to 1-2 liters per hour in dry hot climate
- 30-50 mEq/L Na
- Thirst is primary compensation for this
- Sweat sodium losses can result in hypovolemia
- Burns and exudative skin losses changes the nature of fluid losses resulting in fluid losses more similar to plasma with a variable amount of protein
- Bronchorrhea
- Sequestration into a third space
- Volume Deficiency produced by the loss of interstitial and intravascular fluid into a third space that is not in equilibrium with the extracellular fluid.
- Hip fracture 1500-2000 into tissues adjacent to fxr
- Intestinal obstruction, severe pancreatitis, crush injury, bleeding, peritonitis, obstruction of a major venous system
- Difference between 3rd space and cirrhosis ascities
- Rate of accumulation, if the rate is slow enough there is time for renal sodium and water compensation to maintain balance.
- So cirrhotics get edema from salt retension and do not act as hypovolemia
- Hemodynamic response to volume depletion
- Initial volume deficit reduced venous return to heart
- Detected by cardiopulmonary receptors in atria and pulmonary veins leading to sympathetic vasoconstriction in skin and skeletal muscle.
- More marked depletion will result in decreased cardiac output and decrease in BP
- This drop in BP is now detected by carotid and aortic arch baroreceptors resulting in splanchnic and renal circulation vasoconstriction
- This maintains cardiac and cerebral circulation
- Returns BP toward normal
- Increase in BP due to increased venous return
- Increased cardiac contractility and heart rate
- Increased vascular resistance
- Sympathetic tone
- Renin leading to Ang2
- These can compensate for 500 ml of blood loss (10%)
- Unless there is autonomic dysfunction
- With 16-25% loss this will not compensate for BP when patient upright
- Postural dizziness
- Symptoms
- Three sets of symptoms can occur in hypovolemic patients
- Those related to the manner in which the fluid loss occurs
- Vomiting
- Diarrhea
- Polyuria
- Those due to volume depletion
- Those due to the electrode and acid base disorders that can accompany volume depletion
- The symptoms of volume depletion are primarily related to the decrease in tissue perfusion
- Early symptoms
- Lassitude
- Fatiguability
- Thirst
- Muscle cramps
- Postural dizziness
- As it gets more severe
- Abdominal pain
- Chest pain
- Lethargy
- Confusion
- Symptomatic hypovolemia is most common with isosmotic Na and water depletion
- In contrast pure water loss, causes hypernatremia, which results in movement of water from the intracellular compartment to the extracellular compartment, so that 2/3s of volume loss comes from the intracellular compartment, which minimizes the decrease in perfusion
- Electrolyte disorders and symptoms
- Muscle weakness from hypokalemia
- Polyuria/poly dips is from hyperglycemia and hypokalemia
- Lethargy, confusion, Seizures, coma from hyponatremia, hypernatremia, hyperglycemia
- Extreme salt craving is unique to adrenal insufficiency
- Eating salt off hands ref 18
- Evaluation of the hypovolemic patient
- Know that if the losses are insensible then the sodium should rise
- Volume depletion refers to extracellular volume depletion of any cause, while dehydration refers to the presence of hypernatremia due to pure water loss. Such patients are also hypovolemic.
- Physical exam is insensitive and nonspecific
- Finding most sensitive and specific finding for bleeding is postural changes in blood pressure
- I don’t find this very specific at all!
- Recommends laboratory confirmation regardless of physical exam
- Skin and mucous membranes
- Should return too shape quickly
- Elastic property is called Turgur
- Not reliable is patients older than 55 to 60
- Dry axilla
- Dry mucus membranes
- Dark skin in Addison’s disease Frim increased ACTH
- Arterial BP
- As volume goes down so does arterial BP
- Marked fluid loss leads to quiet korotkoff signs
- Interpret BP in terms of the patients “normal BP”
- Venous pressure
- Best done by looking at the JVP
- Right atrial and left atrial pressure
- LV EDP is RAP + 5 mmHg
- Be careful if valvular disease, right heart failure, cor pulmonare,
- Figure 14-2
- Shock
- 30% blood loss
- Lab Data
- Urine Na concentration
- Should be less than 25 mmol/L, can go as low as 1 mmol/L
- Metabolic alkalosis can throw this off
- Look to the urine chloride
- Figure 14-3
- Renal artery stenosis can throw this off
- FENa
- Mentions that it doesn’t work so well at high GFR
- Urine osmolality
- Indicates ADH
- Volume depletion often associated with urine osm > 450
- Impaired by
- Renal disease
- Osmotic diuretic
- Diuretics
- DI
- Mentions that severe volume depletion and hypokalemia impairs urea retension in renal medulla
- Points out that isotonic urine does not rule out hypovolemia
- Mentions specific gravity
- BUN and Cr concentration
- Normal ratio is 10:1
- Volume depletion this goes to 20:1
- Serum Na
- Talks about diarrhea
- Difference between secretory diarrhea which is isotonic and just causes hypovolemia
- And osmotic which results in a lower electrolyte content and development of hypernatremia
- Talks about hyperglycemia
- Also can cause the sodium to rise from the low electrolyte content of the urine
- But the pseudohyponatraemia can protect against this
- Plasma potassium
- Treatment
- Both oral and IV treatment can be used for volume replacement
- The goal of therapy are to restore normovolemia
- And to correct associated acid-base and electrolyte disorders
- Oral Therapy
- Usually can be accomplished with increased water and dietary sodium
- May use salt tablets
- Glucose often added to resuscitation fluids
- Provides calories
- Promotes intestinal Na reabsorption since there is coupled Na and Glucose similar to that seen in the proximal tubule
- Rice based solutions provide more calories and amino acids which also promote sodium reabsorption
- 80g/L of glucose with rice vs 20 g/L with glucose alone
- IV therapy
- Dextrose solutions
- Physiologically equivalent to water
- For correcting hypernatremia
- For covering insensible losses
- Watch for hyperglycemia
- Footnote warns against giving sterile water
- Saline solutions
- Most hypovolemic patients have a water and a sodium deficit
- Isotonic saline has a Na concentration of 154, similar to that of plasma see page 000
- Half-isotonic saline is equivalent to 550 ml of
isotonic saline and 500 of free water. Is that a typo?
- 3% is a liter of hypertonic saline and 359 extra mEq of Na
- Dextrose in saline solutions
- Give a small amount of calories, otherwise useless
- Alkalinizing solutions
- 7.5% NaHCO3 in 50 ml ampules 44 mEq of Na and 44 mEq of HCO3
- Treat metabolic acidosis or hyperkalemia
- Why 44 mEq and not 50?
- Do not give with calcium will form insoluble CaCO3
- Polyionic solutions
- Ringers contains physiologic K and Ca
- Lactated Ringers adds 28 mEq of lactate
- Spreads myth of LR in lactic acidosis
- Potassium chloride
- Available as 2 mEq/mL
- Do not give as a bolus as it can cause fatal hyperkalemia
- Plasma volume expanders
- Albumin, polygelastins, hetastarch are restricted to vascular space
- 25% albumin can pull fluid into the vascular space
- 25% albumin is an albumin concentration of 25 g/dL compare to physiologic 4 g/dL
- Says it pulls in several times its own volume
- 5% albumin is like giving plasma
- Blood
- Which fluid?
- Look at osmolality, give hypotonic fluids to people with high osmolality
- Must include all electrolytes
- Example of adding 77 mEw of K to 0.45 NS and making it isotonic
- DI can be replaced with dextrose solutions, pure water deficit
- Case 14-3
- Diarrhea with metabolic acidosis
- He chooses 0.25 NS with 44 mEq of NaCl and 44 NaHCO3
- Talks about blood and trauma
- Some studies advocate delaying saline until penetrating trauma is corrected APR about to. Keep BP low to prevent bleeding. Worry about diluting coagulation factors
- Only do this if the OR is quickly available
- Volume deficit
- Provides formula for water deficit and sodium deficit
- Do not work for isotonic losses
- Provides a table to adjust fluid loss based on changes in Hgb or HCTZ
- Says difficult to estimate it from lab findings and calculations
- Follow serial exams
- Serial urine Na
- Rate of replacement
- Goal is not to give fluid but to induce a positive balance
- Suggests 50-100 ml/hr over what is coming out of the body
- Urine
- Insensibles 30-50
- Diarrhea
- Tubes
- Hypovolemic shock
- Due to bleeding
- Sequesting in third space
- Why shock?
- Progressive volume depletion leads to
- Increased sympathetic NS
- Increased Ang 2
- Initially this maintains BP, cerebral and coronary circulation
- But this can decrease splanchnic, renal and mucocutaneous perfusion
- This leads to lactic acicosis
- This can result in intracellular contents moving into circulation or translocation of gut bacteria
- Early therapy to prevent irreversible shock
- In dogs need to treat with in 2 hours
- In humans may need more than 4 hours
- Irreversible shock associated with pooling of blood in capillaries
- Vasomotor paralysis
- Hyperpolarization of vascular smooth muscle as depletion of ATP allows K to flowing out from K channels opening. Ca flows out too leading to vasodilation
- Glyburide is an K-ATP channel inhibitor (?) caused increased vasoconstriction and BP
- Pluggin of capillaries by neutrophils
- Cerebral ischemia
- Increased NO generation
- Which Fluids?
- Think of what is lost and replace that.
- Bleeding think blood
- Raise the hct but not above 35
- Acellular blood substitutes, looked bad at the time of this writing
- Di aspirin cross linked hemoglobin had increased 2 and 28 day mortality vs saline
- Colloids sound great but they fail in RCTs
- SAFE
- FEAST
- Points out that saline replaces the interstitial losses why do we think those losses are unimportant
- Pulmonary circulation issue
- Pulmonary circulation is more leaky so oncotic pressure less effective there
- Talks about the lungs be naturally protected from pulmonary edema
- Rate of fluid
- 1-2 liters in first hour
- Suggests CVP or capillary wedge pressure during resuscitation
- No refs in the rate of fluid administration section
- Lactic acidosis
- Points out that HCO can impair lactate utilization
- Also states that arterial pH does not point out what is happening at the tissue level. Suggests mixed-venous sample.
References
JCI - Phenotypic and pharmacogenetic evaluation of patients with thiazide-induced hyponatremia and a nice review of this topic: Altered Prostaglandin Signaling as a Cause of Thiazide-Induced Hyponatremia
The electrolyte concentration of human gastric secretion. https://physoc.onlinelibrary.wiley.com/doi/10.1113/expphysiol.1960.sp001428
A classic by Danovitch and Bricker: Reversibility of the “Salt-Losing” Tendency of Chronic Renal Failure | NEJM
Osmotic Diuresis Due to Retained Urea after Release of Obstructive Uropathy | NEJM
Is This Patient Hypovolemic? | Cardiology | JAMA
And by the same author, a textbook: Steven McGee. 5th edition. Evidence-Based Physical Diagnosis Elsevier Philadelphia 2022. ISBN-13: 978-0323754835
The meaning of the blood urea nitrogen/creatinine ratio in acute kidney injury - PMC
Language guiding therapy: the case for dehydration vs volume depletion https://www.acpjournals.org/doi/10.7326/0003-4819-127-9-199711010-00020?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
Validation of a noninvasive monitor to continuously trend individual responses to hypovolemia
References for Anna’s voice of God on Third Spacing : Shires Paper from 1964 (The ‘third space’ – fact or fiction? )
References for melanie’s VOG:
2. excellent review of RAAS in pregnancy: The enigma of continual plasma volume expansion in pregnancy: critical role of the renin-angiotensin-aldosterone system
https://journals-physiology-org.ezp-prod1.hul.harvard.edu/doi/full/10.1152/ajprenal.00129.2016
3. 10.1172/JCI107462- classic study in JCI of AngII responsiveness during pregnancy
4. William’s Obstetrics 26th edition!
5. Feto-maternal osmotic balance at term. A prospective observational study